Neuroimaging in Brain Diagnostics | Common CT and MR Practices Explained
870 likes | 1.09k Vues
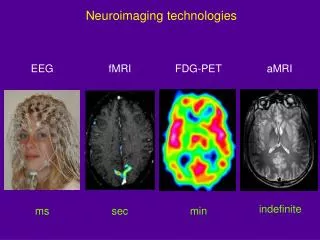
Learn about the use of MR and CT imaging for head trauma and stroke cases. Understand the differences in diagnosing hemorrhagic stroke versus infarct (non-hemorrhagic stroke). Explore how MR imaging offers detailed insights into brain pathology compared to CT scans.

Neuroimaging in Brain Diagnostics | Common CT and MR Practices Explained
E N D
Presentation Transcript
MR generally best tool for imaging the brain • Non-contrast CT still used as first test for 2 common emergency indications: head trauma and stroke • In both cases looking for acute blood which is white relative to brain, because of lipid content of brain
3 trauma cases with blood in meningeal compartments going from superficial to deep: epidural, subdural, and subarachnoid bleeds • Looking for blood collections that create mass effect on brain and need to be evacuated surgically • Usually no mass effect with subarachnoid bleed, but need to consider if subarachnoid bleed was from aneurysm that then caused patient to crash car (which came first)
Stroke: sudden neurologic deterioration on vascular basis (CVA) • Key reason for doing CT is to determine if stroke is hemorrhagic or not. Causes and treatments are different. May give thrombolytic emergently for acute infarct, but not for bleed • How soon does hemorrhagic stroke show up on CT? : Immediately! • Following case is typical hypertensive basal ganglia bleed
Next case is non-hemorrhagic left occipital stroke (infarct) • How soon does infarct show up on CT?: Depends on the size. Large one may have subtle swelling in 6 hours, but smaller one may take a couple days. Therefore, emergent head CT is done to see if patient has bleed or not, not to necessarily to see an infarct • Infarct becomes low density as edema develops
This is the same patient with infarct shown on MR (first 2 series: T1- and T2-weighted) • As opposed to CT, MR can measure more than one variable, e.g., T1 and T2, so if lesion not well seen on one sequence, may be better seen on another. CT can measure only one variable, X-ray attenuation • MR more sensitive to soft tissues differences than CT. Can see edema of infarct sooner. • Water is dark on T1 and bright on T2
Typical MR unit is superconducting magnet which is always on. • Need very strong magnetic field to magnetize hydrogen nuclei. Net vector of magnetization is then tipped by adding RF energy. Precessing vector then creates sine wave signal captured by coils placed around body part of interest. The decay of the signal depends on a couple effects, and the images created can depend more on one factor than the other (T1 or T2)
Same patient with additional common MR sequence (FLAIR) • FLAIR is like T2 sequence, but pure water signal is set to zero, getting rid of all of the bright signal from CSF. The edema (water) in infarct stays bright since it is in the brain with a different surrounding molecular environment, and therefore a different signal than protons in pure water (CSF). It makes the visual search for pathology easier.
MR signal depends on another variable, motion. The basilar artery on the T2 image is a black dot anterior to the brain stem. Although there is a lot of water in the artery, and it might be expected to be bright on T2, it has a flow void because the protons have moved out of the imaging volume and haven’t gone through entire process of signal generation. • Therefore, can do MRA without contrast • Diffusion-weighted scan signal depends on microscopic motion/diffusion. Infarct is bright on DW because acute ischemia causes shift of water from extracellular space to intracellular where water can’t move as much. There is less of a “microscopic flow void” and infarct is bright. This occurs much earlier than edema, and is sensitive and fairly specific for acute infarct. • Following is the very commonly performed diffusion-weighted sequence on the same patient
62-year-old patient with progressive right arm weakness over the last week
3 images are T1, T2, and T1 gadolinium-contrast-enhanced MR • T1 and T2 are very sensitive to pathology, but often not specific, since most pathologies all over body are dark on T1 and bright on T2, like infarct, because they have increased water content • T2 sequences good for screening because most pathologies are bright • Gadolinium adds specificity. There are 2 enhancing (therefore solid) masses. They light up because Gd doesn’t cross blood-brain barrier into normal brain, but does enter tumor extracellular space • Brain mets from lung CA, most common malignancy presenting with brain mets
70-year-old female with sudden severe low back pain when lifting and turning to empty a heavy garbage can
Sounds like osteoporotic compression fx • Well shown on plain X-ray
36 year-old-patient with severe left leg sciatica not responding to physical therapy, and now with calf weakness
Imaging not usually indicated initially for sciatica, because will usually resolve with conservative treatment (PT, meds) • Do imaging if conservative Rx fails or if neurologic damage develops (weakness, loss of reflex) • MR exam of choice because it has excellent soft tissue contrast. CT has very high spatial resolution for high-contrast tissues (like nodules in lung or fracture in bone), but not as good for soft tissues • MR shows L4-5 disc protrusion compressing left L5 nerve root.
67-year-old patient with bilateral leg pain increasing with distance walked (non-smoker, no diabetes, normal pedal pulses)
History suggests claudication, but also suggests not vascular • This is spinal claudication caused by spinal stenosis
Severe spinal stenosis on CT due to facet joint degenerative disease and hypertrophy • CT will show bony stenosis well, but won’t show soft tissue component as well as MR