Download
1 / 100
1.03k likes | 1.46k Vues
Bakhshaee M, MD Rhinologist Assistant Professor of Mashad University of Medical Sciences. Nose and Paranasal Sinuses. Course Plan. Four sessions: Anatomy, Physiology, and Immunology of the Nose, Paranasal Sinuses, and Face

E N D
Bakhshaee M, MD Rhinologist Assistant Professor of Mashad University of Medical Sciences Nose and Paranasal Sinuses
Course Plan • Four sessions: • Anatomy, Physiology, and Immunology of the Nose, Paranasal Sinuses, and Face • History and Clinical Examination of the Nose; Tumors of the External Nose and Face • Malformations and common disorders of the Nose, Paranasal Sinuses, and Face • Inflammations of the External Nose, Nasal Cavity, and Facial Soft Tissues Estimated time for each session is 100 min
Session’ Items • Including: • Initial assessment: 10 min • Lesson delivery: 60 min • Discussion: 15 min • Question and problems of previous session: 10 min • A brief talking on next session: 5 min
Session 1 Anatomy, Physiology, and Immunology of the Nose, Paranasal Sinuses, and Face
Anatomy, Physiology, and Immunology of the Nose, Paranasal Sinuses, and Face • Basic Anatomy of the Nose, Paranasal Sinuses, and Face • Morphology of the Nasal Mucosa • Basic Physiology and Immunology of the Nose
Facial Skin and Soft Tissues The relaxed skin tension lines (RSTLs): Scars can be made less conspicuous by taking these tension lines into account The aesthetic units of the face: an important consideration in the treatment larger soft-tissue defects
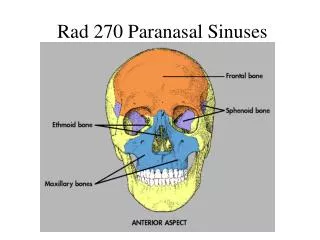
The Facial Skeleton Knowing the various components of the bony facial skeleton and their relationship to one another is important in trauma management and also in the diagnosis and treatment o inflammatory diseases of the facial skeleton and their complications.
Nasal Cavities Nasal Vestibule Nasal Septum Nasal Valve Lateral nasal Wall Choana
Lateral Nasal Wall Bony Structure: Maxilla Ethmoid Palatine Inferior Turbinate Sphenoid Functional apparatus: Turbinate Meatus Sinus ostia Nasolacrimal duct orifice
Nasal Cavities Roof: Cribriform palate Ethmoid fovea Floor: Hard palate Maxilla (Ant) Palatine (Pos)
Paranasal Sinuses Air-filled cavities that communicate with the nasal cavities All but the sphenoid sinus are present as outpunching of the mucosa during embryonic life, but except for the ethmoid air cells, they do not develop into bony cavities until after birth.
Maxillary Sinus Medial: Lateral nasal wall Superior: Orbital floor Posterior: Pterygopalatine fossa Inferior: Alveolar ridge ( root of second premolar and first molar)
Ethmoid air cells Medial: Middle turbinate Superior: Fovea ethmoidalis ( Ant cranial fossa) Posterior: Sphenoid sinus Lateral: Lamina papyruses ( orbit)
Sphenoid Sinus Inferior: Nasopharynx Superior: Ant and middle cranial fossa , Sellae tursica Posterior: Clivus and posterior cranial fossa Lateral: Optic nerve Internal carotid Cavernous sinus
Frontal Sinus Inferior: Orbital roof Posterior: Anterior cranial fossa
Nerve Supply Innervation
AnatomyExternal Muscular attachments
Morphology of the Nasal Mucosa Mucus: Squamous epithelium Respiratory Mucosa Olfactory Mucosa Respiratory Mucosa: Epithelium Lamina Properia: Venous erectile tissue Nasal glands Immunocompetent cells Olfactory Mucosa: primary olfactory center ( olfactory bulb) secondary olfactory center (olfactory cortex) tertiary olfactory centers (including the hippocampus, anterior insular region, and reticular formation)
Basic Physiology and Immunology of the Nose Nose is of major importance in conditioning the air before it reaches the lower airways
Physical Principles of Nasal Airflow Nasal Air Flow Laminar vs Turbulent Nasal Cycle Regulate by autonomic nervous system 80% of human each 2 hours
Conditioning of the Inspired Air Humidification Temperature regulation
Protective Functions of the Nasal Mucosa Nonspecific Defense Mechanisms Mechanical defenses (mucociliary apparatus) Nonspecific protective factors (Interferon, Proteases, Protease inhibitors , Lysozyme Antioxidants) Cellular defenses (phagocytic cells) Specific Immune Responses Humoral immune response Cellular immune response The endothelial cells The epithelial cells
Speech Production Various organ systems are involved in the production of voice and speech: • Glottis, • Supraglottic vocal tract, • Central nervous system must be coordinated in order to produce a normal voice sound • Hyponasal speech (rhinophonia clausa) : occurs when these segments contribute less to sound production as a result of partial or complete nasal obstruction or mass lesions in the nasopharynx • Hypernasal speech (rhinophonia aperta):develops when the nasopharynx and nasal cavities over contribute to sound production. cleft palate, velar palsy due to various causes
Olfaction • The human olfactory system consists of • Intranasal olfactory mucosa • Primary olfactory center • Secondary olfactory center • Tertiary olfactory center • The precise sequence of events that are involved in olfaction is still uncertain.
Questions • Name the main the nasal septum structure. • Name the functions of the nose? • The major artery of the nose is …. • Sphenoid sinus is drained to …. • Orbital cellulitis is seen often due to … sinus involvement.
Session 2 History and Clinical Examination of the Nose; Tumors of the External Nose and Face
History • Patients should be given an opportunity to describe their complaints “in their own words,”
Common Complains • Nasal obstruction • Discharge • Epistaxis • Specific allergy history • Headaches • Olfactory dysfunction • Facial pressure or pain
Nasal airwayobstruction • Acute and chronic rhinitis (e.g., allergic, atrophic) • • Sinusitis • • Deviated septum (congenital, acquired) • • Nasal pyramid fracture • • Septal perforation • • Nasal polyps • • Cephalocele • • Adenoids • • Tumors of the nose, paranasal sinuses, and nasopharynx • • Foreign bodies (especially in small children) • • Drugs • Adverse effects: oral contraceptives, antihypertensive agents (e.g., reserpine, propranolol, hydralazine), antidepressants (e.g., amitriptyline) • Drug abuse: e.g., oxymetazoline , phenylephrine
Olfaction Disturbance • Transport of odorants • Nasal obstruction Deviated septum, mucosal • swelling, polyps, tumor • Scar tissue occluding the olfactory groove • After intranasal surgery • Perception: damage to the olfactory epithelium caused by: • Toxic substances SO2, NO, ozone, • Heavy metals, varnishes • Drugs • Viral infections Influenza • Radiotherapy (rare) • Stimulus conduction and processing • Avulsion of filaolfactoria Skull base fracture • Aplasia of the olfactory bulb (rare) • Kallmann syndrome • Injury to olfactory centers • Contusion or hemorrhage due to head injury • Neurodegenerative diseases • Alzheimer disease, • Parkinson disease, • Diabetes mellitus • Olfactory hallucinations after epileptic seizures, in schizophrenia
Clinical Examination • Inspection • Mouth breathing • Shape of the external nose • Skin changes such as erythema
Exam,con • Palpation • Useful for detecting bony discontinuities • In patients with suspected neuralgias
Anterior Rhinoscopy • To evaluate the nasal vestibule and the anterior portions of the nasal cavity
Posterior Rhinoscopy • Posterior rhinoscopy was formerly done to evaluate the nasopharynx and posterior nasal cavity (choanae, posterior ends of the turbinates, posterior margin of the vomer) • Endoscopy is commonly used to examine this region
Nasal Endoscopy • Nasal endoscopy has become the most important and rewarding clinical examination method in rhinologic diagnosis
Nasopharynx • First the examiner advances the endoscope into the nasopharynx and inspects: • Eustachian tube orifice • Torus tubarius • Posterior pharyngeal wall • Roof of the nasopharynx
Ostiomeatal unit • Nasal endoscopy is particularly useful for evaluating the ostiomeatal unit
Testing Nasal Patency • Nasal Patency: • Hold a reflective metal plate under the nose • Holding a wisp of cotton in front of each nostril • Active anterior rhinomanometry • Acoustic rhinometry
Allergy Testing • Skin Tests • The total immunoglobulin E (IgE) assay • Nasal provocation test
Serologic Tests • The total immunoglobulin E (IgE) assay
Subjective Olfactory Testing • Several types of test substance are used: • Pure odorants that stimulate only the olfactory nerve (coffee, cocoa, vanilla, cinnamon, lavender) • Odorants with a trigeminal component (menthol, acetic acid, formalin) • Substances that also have a taste component (chloroform, pyridine). • Patients with a complete loss of smell (anosmia) cannot perceive pure odorants but can at least sense or taste the other substances.
Objective Olfactory Testing • Objective olfactory testing is far more costly and is generally performed only at large centers
Imaging of the Nose and Paranasal Sinuses • Conventional Radiographs • Computed Tomography (CT) • Magnetic Resonance Imaging • Ultrasonography
Conventional Radiographs • Limited indication these days
Indications • Water projection • Caldwell • Acute inflammation • To evaluate midfacial fractures
Waters Caldwell