Download
1 / 23
350 likes | 1.21k Vues
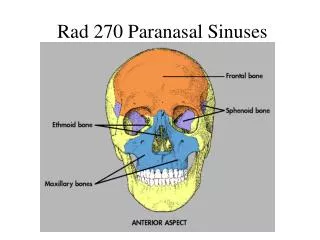
Radiology of Nasal Cavity and Paranasal Sinuses. Radiology. XRAY CT MRI. Normal Anatomy. Drainage system. Lamella: 1) uncinate 2) ethmoidal bulla 3) basal lamella 4) superior turb lamella. Uncinate attachment variations. Agger Nasi. Frontal sinus outflow tract.

E N D
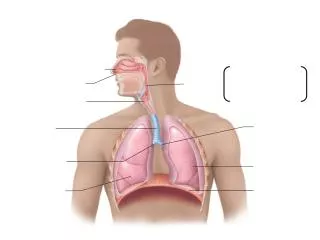
Radiology • XRAY • CT • MRI
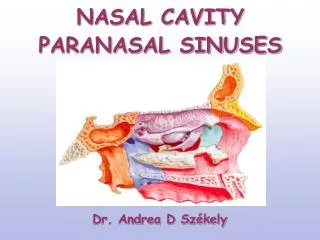
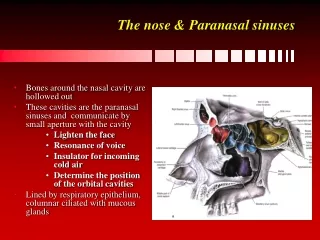
Drainage system Lamella: 1) uncinate 2) ethmoidal bulla 3) basal lamella 4) superior turb lamella
Frontal sinus outflow tract • May be narrowed by agger anteriorly or bulla posteriorly • Frontal cells (Type 1-4) • Frontal recess • Lateral: lamina papyracea • Medial: middle turbinate • Anterior: posterior wall of aggernasi • Posterior: ethmoid bulla
Basal lamella B U L
Other anatomic variations • Concha bullosa • Septal deviations • Paradoxic middle turbinate • convex curvature on the lateral, rather than medial side of the turbinate • Dehiscent lamina • Aerated crista galli • Optic nerve/carotid artery
MRI • Helpful for evaluation of regional and intracranial complications • Detection and staging of neoplastic processes • Improved display between intraorbital and extraorbital compartments • Helpful for diagnosing fungal concretions which show low or no signal on T2 • Helps for evaluation of mucoceles and cephaloceles • Appearance varies with changing concentrations of proteins and free water protons • T2 more “watery”, higher signal • T1 more protein, higher signal • However, once protein content reaches too high signal decreases
Epistaxis • Most common otolaryngologic emergency • Majority idiopathic • 60% of population in their lifetime • Maxillary sinus ostium serves as dividing line between “anterior” and “posterior bleeds”
Endoscopic SPA ligation • Epistaxis controlled in 98% • Locate SPA at level of crista ethmoidalis • Key in surgery is to ligate all branches which can vary
Embolization • Risk of complications: CVA, hemiplegia, ophthalmoplegia, facial nerve palsy, seizures, soft tissue necrosis • Effective only for ECA supply very dangerous for ICA supply due to high risk of blindness • Success rate 71-95% • Complication rate 27%
Anterior ethmoid artery bleeding • Associated with nasoethmoid fractures • Bleeding rarely subsides with conservative measures • Variable position • Always seen between second and third lamellae • Most common site in the suprabullar recess (85%)