VALVULER HEART DISEASE
870 likes | 1.16k Vues
VALVULER HEART DISEASE. Olcay ÖZVEREN, M.D. Aortic Stenosis. Aortic stenosis (AS) is defined as the reduction of the orifice of the aortic valve caused by a failure of the leaflets to open fully during systole.

VALVULER HEART DISEASE
E N D
Presentation Transcript
VALVULER HEART DISEASE Olcay ÖZVEREN, M.D.
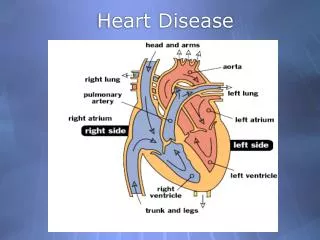
Aortic Stenosis Aortic stenosis (AS) is defined as the reduction of the orifice of the aortic valve caused by a failure of the leaflets to open fully during systole. Left ventricular outflow obstruction most commonly occurs at the aortic valve, however it can occur above the aortic valve (supravalvular) or below the aortic valve as in hypertrophic obstructive cardiomyopathy (HOCM).
The risk factors of calcific AS • Similar to those for vascular atherosclerosis : .elevated serum levels of LDL cholesterol and lipoprotein(a) .Diabetes .Smoking .hypertension.
RheumaticAorticStenosis • Rheumatic AS resultsfromadhesionsandfusionsof thecommissuresandcuspsandvascularization of theleafletsof thevalve ring, leadingtoretractionandstiffening of thefreeborders of thecusps. • Calcificnodulesdevelop on bothsurfaces, andtheorifice is reducedto a smallroundortriangularopening • Therheumaticvalve is oftenregurgitant, as well as stenotic. • Patientswithrheumatic AS invariabilityhaverheumaticinvolvement of the mitral valve .
LV wall stress is directly proportional to myocardial O2 demand, more specifically: O2 demand = wall stress X HR Using the above equation, we can understand the pathologic process that develops over many years in patients with aortic stenosis. As LV pressure slowly increases over time due to worsening aortic stenosis, a parallel increase in LV wall thickness occurs (concentric hypertrophy) in order to maintain the LV wall stress at a constant level (since LV wall stress is an important determinant of myocardial O2 demand). Eventually, the LV is unable to hypertrophy any further, but the LV pressure continues to rise as the aortic stenosis worsens. This leads to a rise in LV wall stress and thus a rise in LV myocardial oxygen demand. When the heart rate increases in response to exertion (heart rate is also a determinant of O2 demand), a significant supply versus demand mismatch occurs resulting in myocardial ischemia and the clinical symptoms of angina.
Symptoms • exertionaldyspnea (LV diastolicdysfunction, with an excessiverise in end-diastolicpressureleadingtopulmonarycongestionandthelimitedabilitytoincreasecardiacoutputwithexercise ) • Angina (precipitatedbyexertionandrelievedby rest. Anginaresultsfromthecombination of theincreasedoxygenneeds of hypertrophiedmyocardiumandreduction of oxygendeliverysecondarytotheexcessivecompression of coronaryvessels ) • Syncope (reducedcerebralperfusionthatoccursduringexertionwhenarterialpressuredeclinesconsequenttosystemicvasodilation in the presence of a fixedcardiacoutput , MAP = CO X TPR) • heartfailuresymtoms
PhysicalExamination • parvusandtarduscarotidimpulse (slow-rising, late-peaking, low-amplitudecarotidpulse .However, in patientswithassociated AR or in olderpatientswith an inelasticarterialbed, systolicandpulsepressuresmay be normal orevenincreased. ) • Thecardiacimpulse is sustainedandbecomesdisplacedinferiorlyandlaterally . • systolicthrill (It is palpatedmostreadily in thesecondrightintercostalspaceorsuprasternalnotchand is frequentlytransmittedalongthecarotidarteries. Itthrill is specific, but not sensitive, for severe AS. )
Auscultation • Theejectionsystolicmurmur"diamond shaped“, crescendo-decrescendo. …Typically is latepeakingandheardbestat thebase of theheart, withradiationtothecarotids. Cessation of themurmurbefore A2 is helpful in differentiationfrom a pansystolic MR murmur. Inpatientswithcalcifiedaorticvalves, thesystolicmurmur is loudest at thebase of theheart, but high-frequencycomponentsmayradiatetotheapex (Gallavardinphenomenon), in whichthemurmurmay be soprominentthat it is mistakenforthemurmur of MR. …A louderandlaterpeakingmurmurindicatesmore severe stenosis. …Whentheleftventriclefailsandstrokevolumefalls, thesystolicmurmur of AS becomessofter; rarely, it disappearsaltogether. Theslowrise in thearterialpulse is moredifficulttorecognize Theintensity of thesystolicmurmurvariesfrombeattobeatwhentheduration of diastolicfillingvaries, as in AF orfollowing a prematurecontraction. Thischaracteristic is helpful in differentiating AS from MR, in whichthemurmur is usuallyunaffected. • Splitting of thesecondheartsound helpful in excludingthediagnosis of severe AS becausenormal splittingimpliesthe AV leafletsareflexibleenoughtocreate an audibleclosingsound (A2). . A S4 heart sound is also often present due to the severe concentric left ventricular hypertrophy that develops in aortic stenosis. If a S3 heart sound is present, then significant systolic dysfunction has developed which is common in end stage aortic stenosis.
Diagnostic Evaluation Modalities • Echocardiography (definition of valve anatomy, including the cause of AS and the severity of valve calcification, evaluation of LV hypertrophy and systolic function, mean transaortic pressure gradient with calculation of the ejection fraction, and for measurement of aortic root dimensions and detection of associated mitral valve disease.) • Cardiac Catheterization and Angiography • Computed Tomography • Cardiac MR
Clinical Outcome Asymptomatic Symptomatic • 2 years in patientswithheartfailure . • 3 years in thosewithsyncope • 5 years in thosewithangina
Theaverage rate of hemodynamicprogression : annualdecrease in aorticvalvearea of 0.12 cm2/year an increase in aortic jet velocity of 0.32 m/sec/year an increase in meangradient of 7 mm Hg/year. Exercise test is helpful : • Symptoms on treadmillexercise • a decrease in bloodpressurewithexertion • An elevated BNP levelmay be helpfulwhensymptomsareequivocalorwhenstenosisseverity is onlymoderate.
Management • Symptomaticpatientswith severe AS areusuallyoperativecandidatesbecausemedicaltherapy has littletooffer . • Medicaltherapymay be necessaryforpatientsconsideredto be inoperable , HF , HT, CAD. • Diüretics ,ACE inh. ,Statins, • DC Cardiversion in AF
Valvular Disease • calcific AR • infective endocarditis • trauma • congenitally bicuspid valve • Rheumatic fever • SLE • rheumatoid arthritis • ankylosing spondylitis • Takayasu disease, • Whipple disease, • Aortic Root Disease • Marfan syndrome; • aortic dilation related to bicuspid valves • aortic dissection, • osteogenesis imperfecta, • syphilitic aortitis, • ankylosing spondylitis, • the Beh?et syndrome, • giant cell arteritis, • systemic hypertension
ClinicalPresentation • Most of thepatients remaining asymptomatic for a long period of time early in disease. • exertionaldyspnea • Angina(Itmay occur in the absence of atherosclerotic coronary disease since the low diastolic pressures in severe aortic regurgitation compromise coronary filling and the LVH results in increased oxygen demand) • Syncope • heartfailure(Signs of left and right heart failure occur late in disease. Left heart failure results in symptoms related to the low cardiac output. The pressure increases in the left heart transmit to the lungs causing pulmonary edema and shortness of breath. ) • Other symptoms related to low cardiac output include fatigue, weakness and in extreme cases, cardiac cachexia can occur.
PhysicalFindings Quincke'sPulse: Capillarypulsationvisible on thefingernailbedsortips Musset'sSign: Headbobbingwitheachheartbeat Müller’sSign: Systolicpulsation of theuvula Corrigan’sPulse: Water-hammerpulse. Rapiddistentionandcollapse of arterielpulse Hill’sSign: Poplitealcuffpressuremorethan 60 mmHgabovebrachialcuffpressure Duroziez’sSign:To-and-fromurmuroverthefemoralarterywiththearterycompressed Traube’ssign: Pistol-shotsounds. Prominentsystolicanddiastolicsoundsoverthefemoralarteries Increasedpulsepressure (SBP increasesand DBP decreases.)
Shelly's sign: Pulsation of the cervix. Rosenbach's sign: Hepatic pulsations. Becker's sign: Visible pulsation of the retinal arterioles. Gerhardt's sign (aka Sailer's sign):Pulsation of the spleen in the presence of splenomegaly. Mayne's sign:A decrease in diastolic blood pressure of 15 mmHg when the arm is held above the head (very non-specific). Landolfi's sign: Systolic contraction and diastolic dilation of the pupil.
DiastolicMurmurIn AR • In moderate AR, a relatively loud early desending diastolic murmur is heard. • With more severe AR, the murmur becomes longer, and will usually decrease in intensity. • The classic murmur caused by the regurgitant flow is best heard along the lower left sternal border. In some cases (Marfan’s Syndrome, VSD w/AR , aortic dissection or aneurysm) it is best heard at the right sternal border. • A lower-pitched mid-diastolic murmur is heard over apex this indicates what is called an Austin Flint murmur which indicates severe AR. (The murmur is not the regurgitant flow over the aortic valve, but rather vibrations in a restricted Mitral Valve when the left atrium empties and is met with the opposite flow from the aortic valve.) • In addition to the diastolic murmur(s), a systolic flow murmur like in aortic stenosis may be heard. This is not necessarily indicating a calcified valve, as the increased velocity resulting from ventricular overload will also cause flow vibrations)
Diagnostic Evaluation Modalities • Echocardiography (bicuspidvalve, thickening of thevalvecusps, othercongenitalabnormalities, prolapse of thevalve, a flailleaflet, orvegetation ) • Electrocardiography(leftaxisdeviationand a pattern of LV diastolicvolumeoverload, characterizedby an increase in initialforces (prominent Q waves in leads I, aVL, and V3 through V6) and a relativelysmallwave in lead V1 ) • Radiography • CardiacMagneticResonanceImaging • Angiography
Disease Course asymptomatic symptomatic
Management • MedicalTreatment :There is no specifictherapytopreventdiseaseprogression in chronic AR. • Systemicarterialhypertension, should be treatedbecause it increasestheregurgitantflow; vasodilatingagentssuch as ACE inhibitorsor ARB arepreferred, and beta-blockingagentsshould be usedwithgreatcaution. • Chronicmedicaltherapymay be necessaryforsomepatientswhorefusesurgeryorareconsideredto be inoperablebecause of comorbidconditions. Thesepatientsshouldreceive an aggressiveheartfailureregimenwith ACE inhibitors (andperhapsothervasodilators), digoxin, diuretics, and salt restriction; beta blockersmayalso be beneficial.
Acute Aortic Regurgitation • Causes: infectiveendocarditis, aorticdissection, trauma • Thecharacteristicfeatures of acute AR aretachycardiaand an increase in LV diastolicpressures. • Thesuddenincrease in LV fillingcausesthe LV diastolicpressuretoriserapidlyaboveleftatrialpressureduringearlydiastole . • Prematureclosure of the mitral valve, togetherwithtachycardiathatalsoshortensdiastole, reducesthe time intervalduringwhichthe mitral valve is open. • Thetachycardiamaycompensateforthereducedforwardstrokevolume, andthe LV andaorticsystolicpressuresmayexhibitlittlechange. • Acute severe AR maycauseprofoundhypotensionandcardiogenicshock . • Weakness, severe dyspnea, andprofoundhypotensionsecondarytothereducedstrokevolumeandelevatedleftatrialpressure .
PhysicalExamination • tachycardia, severe peripheralvasoconstriction, andcyanosis, andsometimespulmonarycongestionandedema. • S1may be softorabsentbecause of prematureclosure of the mitral valve, andthesound of mitral valveclosure in midorlatediastole is occasionallyaudible. Closure of the mitral valvemay be incomplete, anddiastolic MRmayoccur • Theearlydiastolicmurmur of acute AR is lowerpitchedandshorterthanthat of chronic AR because as LV diastolicpressurerises, the (reverse) pressuregradientbetweenthe aorta andleftventricle is rapidlyreduced.
Echocardiography:Inacute AR theechocardiogramreveals a dense, diastolicDopplersignalwith an end-diastolicvelocityapproachingzeroandprematureclosureanddelayedopening of the mitral valve. LV size andejectionfractionare normal. • Electrocardiography:Inacute AR, the ECG mayormay not show LV hypertrophy, depending on theseverityandduration of theregurgitation. However, nonspecific ST-segmentand T wavechangesarecommon. • Radiography :Inacute AR, there is oftenevidence of markedpulmonaryvenoushypertensionandpulmonaryedema.
Management • Earlydeathcausedby LV failure is frequent in patientswithacute severe AR despiteintensivemedicalmanagement, promptsurgicalintervention is indicated. • Even a normal ventriclecannotsustaintheburden of acute, severe volumeoverload. • Whilethepatient is beingpreparedforsurgery, treatmentwith an intravenouspositiveinotropicagent (dopamineordobutamine) and/or a vasodilator (nitroprusside) is oftennecessary. • Inhemodynamicallystablepatientswithacute AR secondarytoactiveinfectiveendocarditis, operationmay be deferredtoallow 5 to 7 days of intensiveantibiotictherapy . However, AVR should be undertaken at theearliestsign of hemodynamicinstabilityorifechocardiographicevidence of diastolicclosure of the mitral valvedevelops.
Etiology • RheumaticFever • Congenital Mitral Stenosis
Pathophysiology • Increasedleftatrialpressure • Pulmonaryvasoconstriction • PulmonaryHypertension • RightVentricularFailure • Decreasedcardiacoutput
Symptoms • Fatigue • Palpitations • Cough • Chestpain • SOB • Left sided failure • Orthopnea • PND • Exercisedyspnea • Palpitation • Hoarseness (Ortner’ssyndrome • Afib • Systemic embolism "Blue toe syndrome“, stroke • Pulmonary infection • Hemoptysis due to sudden rupture of a bronchial vein. This phenomenon is termed "pulmonary apoplexy". • Right sided failure • Hepatic Congestion • Edema